The simple answer is that bipolar disorder can occur without psychosis. The paper that opens the other answer is titled "Differences in resting-state functional magnetic resonance imaging functional network connectivity between schizophrenia and psychotic bipolar probands and their unaffected first-degree relatives." (Emphasis mine.)
You can also have (unipolar) depression with psychotic symptoms. And its status is (and has been) equally iffy:
There has been a long-standing discussion as to whether psychotic depression is a distinct syndrome or simply represents a severe form of depression. Much of the debate stems from the fact that in DSM-II, published in 1968, “psychosis” meant severe and did not mean being out of touch with reality or having delusions or hallucinations. In 1970, Gerald Klerman and Eugene Paykel published an influential article that stated that in depression, there was a smooth continuum from mild outpatient depression to severe depression requiring inpatient hospitalization without any demarcation points. Observations that psychotic depressed patients differed from nonpsychotic patients in their response to pharmacological treatments led investigators to focus on more clearly defining this distinct clinical entity.
In 1992, as Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV was being planned, a strong argument was made in the American Journal of Psychiatry that there was sufficient evidence at that time from studies of clinical characteristics and symptoms, biology, family history, course and outcome, and treatment that psychotic depression should be a distinct illness in DSM-IV, separate from major depression. The American Journal of Psychiatry article led to a position paper submitted to the DSM-IV Work Group on mood disorders. The DSM-IV Work Group on mood disorders agreed that the clinical relevance of specifically designating patients with psychotic depression was high and considered 2 options: (1) to continue the classification as in DSM-IIIR designating psychosis as decimal point under the severity code and (2) to designate psychotic depression as a separate syndrome “major depression with psychotic features.” After much deliberation, the work group recommended the first option although it recognized it was less than optimal. Thus, in DSM-IV and DSM-IV text revision, psychotic depression remained as a subclassification of major depressive disorder.
Similarly, in the International Classification of Diseases, 10th revision (ICD-10), psychotic depression is classified as a subtype of severe depression. Arguments that psychotic depression meets the criteria for a valid psychiatric syndrome due to its distinct clinical presentation, neurobiology, heritability, prognosis, and treatment response continue to be made with the hope that this will change in ICD-11.
In DSM-V, psychotic depression will remain as a subclassification of major depressive disorder. However, in DSM-V, psychotic features will be separated from the severity rating, and major depressive disorder with psychotic features will not necessarily need to be classified as “severe.” This is a change from DSM-IV. Moreover, in DSM-V, a hierarchy giving precedence to mood-incongruent features is being introduced to allow classification of cases in which mood-congruent and mood-incongruent psychotic features coexist.
Sorry for the rather long quote, but I cannot summarize the controversy of psychotic depression in much less than that.
And to get back to bipolar, DSM-5 split the mood section (one chapter in DSM-IV) into two Depressive and Related Disorders and Bipolar and Related Disorders. They actually located Bipolar in-between Depressive and Schizophrenia Spectrum and Related Disorders
in recognition of their place as a bridge between the two diagnostic classes in terms of symptomatology, family history and genetics
(DSM-5, p. 123)
And if you wonder why this progression, here's some correlational epidemiology
A diagnosis of BPI [bipolar I] disorder was strongly predictive of psychotic features during depression compared to MDDR [major depressive disorder] (odds ratio [OR] = 4.61, p < 0.0005). Having bipolar II compared to MDDR was not predictive of psychosis (OR = 1.05, p = 0.260), nor was having a family history of BPI in MDDR subjects (OR = 1.20, p = 0.840).
And one interesting thing is that in practice, the presence of psychosis makes the diagnosing psychiatrist significantly depart from the DSM:
However, the question of where to place psychotic symptoms within the framework of clinical diagnosis is still confusing. Meyer and Meyer (2009) sought to examine this issue using identical vignettes of a clinical presentation adjusted only for the presence of auditory hallucinations (more commonly associated with psychotic disorders) and the decreased need for sleep (one possible symptom of mania) to evaluate how actual psychiatrists would diagnosis and what subsequent treatment they would recommend. Although the vignette was written to clearly present a patient with mania warranting a diagnosis of Bipolar Disorder (DSM-IV criteria), almost half of the psychiatrists gave an inappropriate diagnosis (45% total; 41.5% psychotic disorder, 3.5% other diagnosis), with a manic episode diagnosed by 37.3% of the psychiatrists and bipolar affective disorder diagnosed by 16.9% of the psychiatrists
as noted in "Historical Underpinnings of Bipolar Disorder Diagnostic Criteria
" which is actually a very good read for the historical basis of the distinction (it started with the Kraepelian dichotomy), much more than I can hope to convey here.
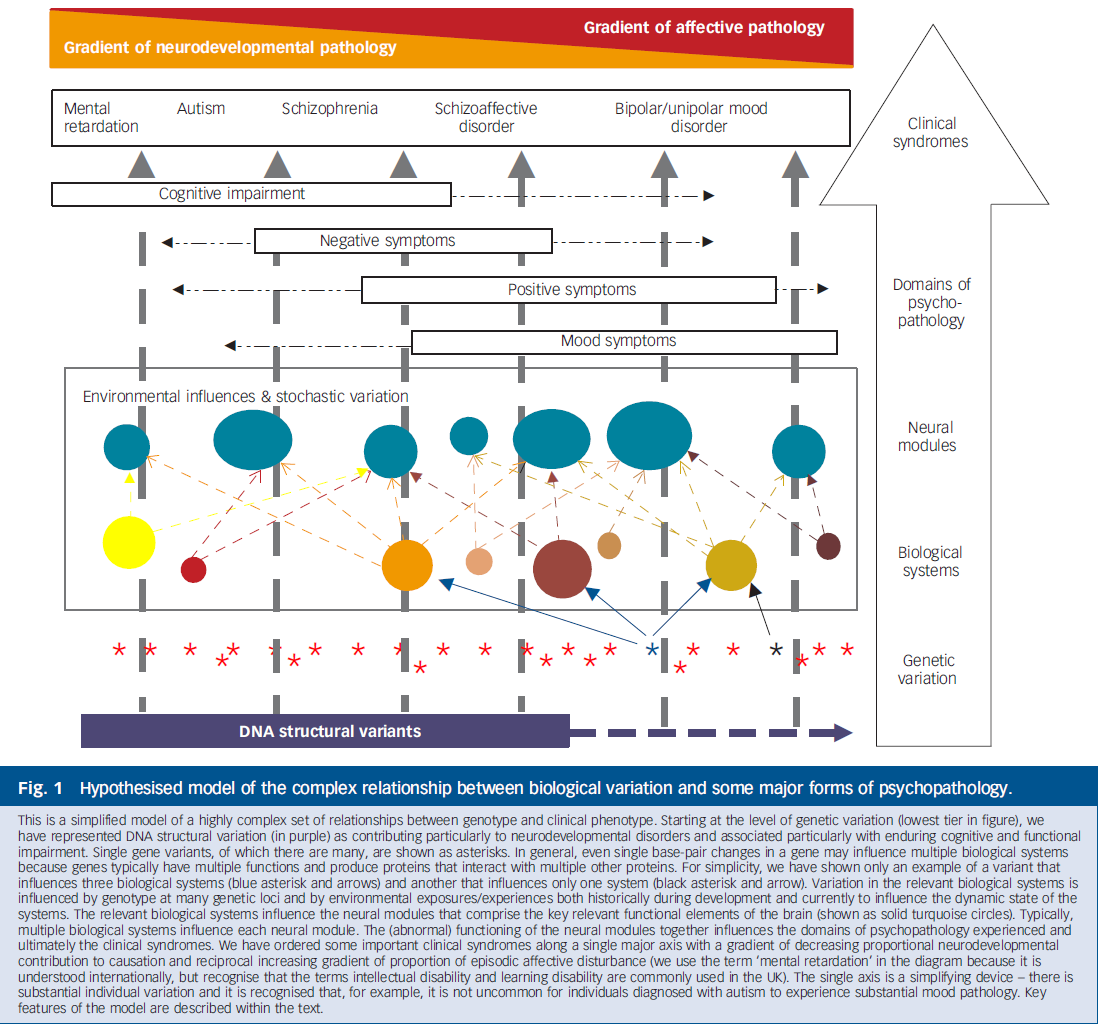
What I will say is that the blurring distinction that the DSM-5 sorta acknowledged has been proposed much more vigorously by some researchers. In particular, Craddock "going" paper was one of my favorite papers some years ago, proposing an even more daring overlap, with cognitive issues of schizophrenia overlapping autism.
Alas, the quest for biomarkers in psychiatry is still in its infancy.
Also, while the DSM (IV) clearly defined bipolar as a mood disorder, they don't say that schizophrenia is a thought disorder, so I'm not sure what you based that on. Science Direct has a page with a lot definitions of schizophrenia excerpted from (recent) books, and none define it a thought disorder although one (Sontheimer) does say that it is
a collection of symptoms that are dominated by psychosis. However, symptoms also include deficits in thinking, behavior, and affect [...]".
Another (Benson) says
its defining symptoms are typically delusions and hallucinations in the absence of extreme emotion. Cognitive impairment or thought disorder is also considered a cardinal symptom.
On the other hand, the NHS does have a page on which it equates psychosis with thought disorder in the title. I guess the specialists don't consider the concepts synonymous, but for the general public... some let that slide.
Bipolar is regarded as a mood disorder.- Depends on whom you ask. What defines amood disorder? What defines athought disorder? What defines anillness? In all honesty, I don't think this is answerable given the current state of psychiatric science, but I'd be happy to be proven wrong... $\endgroup$