Here are a few thoughts:
Work out whether the construct has ceiling effects or whether it is a measurement issue: You need to consider whether people actually discriminate between the rated objects.
Multiple items per rated object: For each medical treatment you could ask participants to answer several questions. You could then take the mean of their responses for the items to get an overall rating of each treatment for each participant. This increases the number of possible scores and should also increase the reliability of measurement.
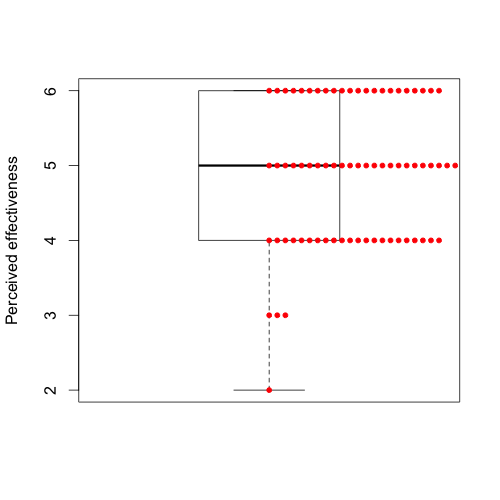
Is the aim to measure the group property or an individual property: For example, if you are aiming to get a measure of the degree to which a group considers a treatment effective, then by averaging over many individuals you should get nuanced measure. So even if people are generally answering 4,5, and 6, one treatment will have more 4s and 5s and another might have more 5s and 6s. The result is that the mean of such ratings will still be nuanced measure, and you can then say things like one treatment having a mean of 4.5 and another having a mean of 5.5, and so on. So in that sense, you can still compare group-level opinions of effectiveness.
Forced choice or ranking format: You could adopt a forced choice or ranking format where participants are asked to rank or make some form of comparative assessment of the relative effectiveness of a set of treatments. This has pros and cons. It will obviously give you a good understanding of perceptions of relative effectiveness, but you will not have information on how effective they perceive the treatments relative to a general standard of effectiveness.
Change the response scale: There are many choices for response scales. You can add more scale points (e.g., go to 7 or 10 point scale). You could even design a scale that is not balanced, so you make more distinctions of effectiveness. Personally, I think you need a principle to govern your choice of scale. A good general rule is to talk to people doing the rating and find out what words they use to describe the effectiveness of treatments. How many distinctions do they make? What is the difference between ineffective and very ineffective in their mind?
Likert itemand a collection of them being averaged aLikert scale, whereas the value of a person for an item is called ascore. $\endgroup$