I think it's important to clarify that pedophilia is currently classified by the DSM IV as a paraphilia. A paraphilia is as a "recurrent, intense sexually arousing fantasies, sexual urges, or behaviors generally involving non-human objects, the suffering or humiliation of oneself or one's partner, children, non-consenting persons.
The word "paraphilia" is considered by most to be pejorative.
It's interesting to note that until 1973, homosexuality was classified as a paraphilia. It was considered as deviant as pedophilia is currently. Today, homosexuality is classified as a sexual orientation.
The current edition, DSM-IV, categorizes pedophilia as a disorder only if the sexual fantasies or urges involve prepubescent children (defined as 13 or younger), if they last at least six months, if the individual has acted on them, or if they cause marked distress (including legal problems). The DSM-IV also specifies that a person be at least 16 years old and at least five years older than the prepubescent child.
The draft version of DSM-V, now undergoing review, proposes several changes to the diagnosis of pedophilia. One is to expand the definition of this disorder to include hebephilia, an attraction to children who are going through puberty. The hybrid category, pedohebephilia, would consist of the pedophilic type (attracted to prepubescent children, generally younger than 11), the hebephilic type (attracted to pubescent children, usually ages 11 through 14), and the pedohebephilic type (attracted to both). In another significant change, the draft suggests that the use of pornography depicting prepubescent or pubescent children for six months or longer should be considered a symptom of pedohebephilia.
The key points the article makes are these:
- Pedophilia is a sexual orientation and unlikely to change. Treatment
aims to enable someone to resist acting on his sexual urges.
- No intervention is likely to work on its own; outcomes may be better
when the patient is motivated and treatment combines psychotherapy
and medication.
- Parents should be aware that in most sexual abuse cases involving children, the perpetrator is someone the child knows.
Pessimism About Pedophilia - Harvard Mental Health Letter - Harvard Health Publications - Harvard Medical School - July 2010
The article goes on to discuss that regardless of classification (paraphilia versus sexual orientation) the focus on pedophilia will have to be on treatment to prevent the pedophile from acting out on his/her sexual urges.
Anecdotally, when in a training on community sex offender management probably, oh, five years ago, the trainer classified three main sexual orientations: homosexuality, heterosexuality, and pedophilia. I remember being so taken aback by this, as I had never even remotely thought of pedophilia as a sexual orientation. In this training, bisexuality was not represented as a sexual orientation, but a note was made of it between homosexuality and heterosexuality on the triangle-shaped chart the trainer was using.
According to the Wikipedia's entry on sexual orientation, the American Psychiatric Association (APA) has stated, "some people believe that sexual orientation is innate and fixed; however, sexual orientation develops across a person's lifetime". The APA also says that "most people experience little or no sense of choice about their sexual orientation". Wikipedia - Sexual Orientation Note: the article elaborates, so you might want to read it in its entirety.
I think there is the impression that if pedophilia is classified as a sexual orientation then it is somehow condoning pedophilia. I disagree that this is true. Assigning any sexual orientation is merely a classification; it just so happens that pedophilia would be, technically, a criminal sexual orientation. I personally see validity in the classification of pedophilia as a sexual orientation, having had a good deal of training that focuses on sex offenders, and pedophiles in particular most of the time. That said, I recognize it's a very controversial topic.
Edited to Add: I wanted to update this answer with information about pedophilia as a sexual orientation and the difference between pedophilia and (child) molestation.
First, I want to reiterate regardless of classification (paraphilia versus sexual orientation) the focus on pedophilia will have to be on treatment to prevent the pedophile from acting out on his/her sexual urges. You might be interested in this quick read, No Known Cure.
These statistics are circa 2008 and the source is the trainers from the Colorado Sex Offender Management Board (SOMB). The following chart shows the proposal for classifying pedophilia as a sexual orientation, rather than a paraphilia.
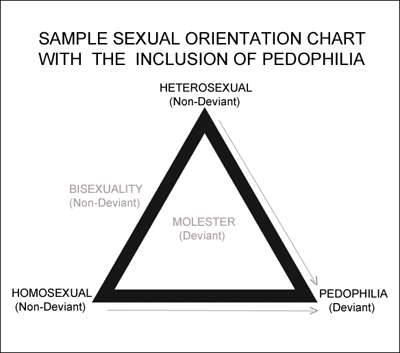
Heterosexuality (non-deviant), homosexuality (non-deviant), and pedophilia (deviant) are defined as the three main sexual orientations. I included bisexuality (non-deviant) as being on the spectrum of sexual orientation, and child molestation (deviant) separate from the sexual orientation spectrum, because molestation is often an opportunistic event rather than an ingrained paraphilia or orientation, and can be non-preferential when it comes to victims.
Why would pedophilia be considered a sexual orientation? (The following is from my notes and I cannot cite specific sources for, say, MRI studies). Pedophiles are sexually attracted to children. It is not a matter of seeing pedophiles who are attracted to the same or opposite sex; it is a matter of being attracted to children in general. Often pedophiles will fixate on prepubescent boys, but if you look at a pedophile's offense history (if they are involved in the criminal justice system) you will find a preponderance of male victims. However, a male-fixated pedophile will also have sexual contact with females when males are not available, which is circumstantial, but the point is pedophiles are sexually aroused by children. Pedophilia is like heterosexuality or homosexuality in that it is innate. It it not a sought after or chosen sexual orientation.
MRI studies have shown there are brain differences in pedophiles; there are areas of the brain that are "missing" or show dark spots or "holes" where gray matter should be. (I'm sorry my notes don't specify which part of the brain is involved)
In comparison, persons who molest a child, but who are not pedophiles, are more opportunistic about their crime(s). As far as sexual orientation goes, a pedophile's orientation is to children; a molester's orientation is to his/her peers, whether heterosexual or homosexual. A pedophile's attraction to children is permanent; a molester's is temporary. The average number of pedophiles who had sexual contact with a child by the age of 19 or younger is 74%; the average number of molesters who had sexual contact with a child by the age of 19 or younger is 57%. The average victim target for pedophiles are males under the age of 13; for molesters, the average target are females approximately the age of 13. Pedophiles are typically not in a relationship or marriage, or are in a marriage of convenience; molesters are typically in a relationship or marriage.
Yet, in opposition to the position that pedophilia is a sexual orientation, there are also statements like this from the SOMB, the same board that provided the training on pedophila as a sexual orientation. Go figure! Anyhow, it says:
Sexual offenses are defined by law and may or may not be associated with or accompanied by the characteristics of sexual deviance which are described as paraphilias. Some sex offenders also have co-existing conditions such as mental disorders, organic disorders, or substance abuse problems.
Many offenders can learn through treatment to manage their sexual offending behaviors
and decrease their risk of re-offense. Such behavioral management should not, however,
be considered a “cure” and successful treatment cannot permanently eliminate the risk
that sex offenders may repeat their offenses.
No Known Cure Position Paper -- Colorado Department of Safety, Division of Criminal Justice, Sex Offender Management Board
I hope this information is useful and not just a lot of jargon to wade through.
Edited to Add: Per your request, a couple paragraphs on paraphilias and mental disorders. Currently, the DSM-IV-TR classifies paraphilia as an Axis I mental disorder (you will also find mental illnesses on Axis I, such as mood disorders, schizophrenia, anxiety disorders, and dysthymia or unipolar depression). The DSM-IV-TR does differentiate between a latent paraphilia, consenting adults engaging in sexual activity that includes paraphilic interest(s), and an active paraphilia in which harm is caused to another person. It is only the latter that is classified as a mental disorder. Is it inherently a mental disorder to have a paraphilia? No. It becomes a mental disorder when acting upon one's paraphilia causes victimization and harm to another person.
Interestingly, some studies have found a solid co-morbidity of paraphilia and other Axis I mental illnesses. For example, A DSM-IV Axis I comorbidity study of males (n = 120) with paraphilias and paraphilia-related disorders (US National Library of Medicine, National Institute of Health). One interesting statistic from the aforementioned paper: The prevalence of any ADHD in the sex offender paraphiliacs was 43.3%, and nearly 25% of offenders were diagnosed with ADHD-combined subtype. Of course one sentence is out of context, so I encourage you to read the abstract in full. As a major symptom of ADHD is impulsivity, I found it a fascinating correlation.